Author
India is on an ambitious path to eliminate malaria by 2030, and we seem to have made some progress. With improved surveillance and access to diagnosis and medicines, the number of malaria deaths in the country has reduced, the World Health Organization (WHO) and the Commonwealth Malaria Report show.
However, while cases have dropped significantly in the past decade, since 2021, number of reported malaria cases have seen a slight uptick. This presents unique challenges in high-burden states like Odisha and Chhattisgarh, where cases have risen by up to 170% in the last 4 years.
This World Malaria Day, First Check looks at India’s malaria burden, and the plans to eliminate the vector borne disease in high burden states.
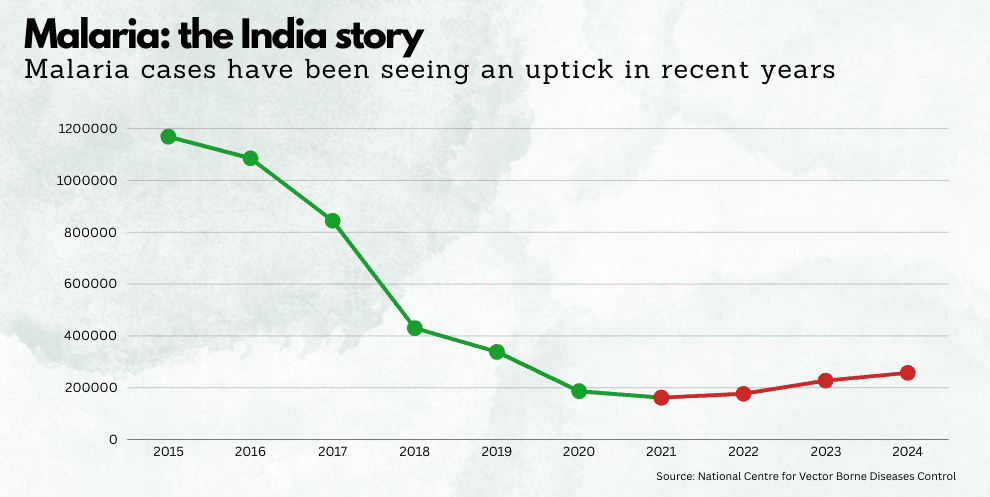
Malaria: the India story
According to the WHO, malaria is a serious, potentially fatal disease transmitted to humans through bites from certain mosquito species. Mostly found in tropical and subtropical regions, it is caused by Plasmodium parasites and is not contagious.
Malaria can be prevented and treated. Preventive measures include protecting against mosquito bites with nets, repellents, or clothing and using prophylactic medications. Effective treatments can halt the progression of mild cases, preventing severe outcomes.
In India, it was considered a public health concern in several parts of the country, until recently. “India exited the HBHI [high burden to high impact] group officially in 2024 due to significant progress in reducing the malaria incidence and mortality observed in its high endemic states,” according to the WHO’s World Malaria Report, 2024.
In the last ten years, between 2015 and 2024, cases of malaria and subsequent deaths have reduced significantly, according to data from the National Centre for Vector Borne Diseases Control. Malaria cases dropped by 78% from about 11.7 lakh cases in 2015, to 2.6 lakh in 2024. Similarly, deaths caused by malaria dropped by 80% from 384 in 2015, to 76 in 2024.
“Intensified surveillance efforts have led to a significant rise in the Annual Blood Examination Rate (ABER)…This strengthened surveillance has ensured early detection, timely intervention, and more effective treatment,” according to a release by the country on India’s malaria elimination progress.
However, in the last 4 years, between 2021 and 2024, cases have seen an upward surge—by about 59% from a low of 1.6 lakh cases. While malaria deaths have not seen an increase during this period, concerns are being raised what this could mean, if cases continue to rise, especially for high burden states.
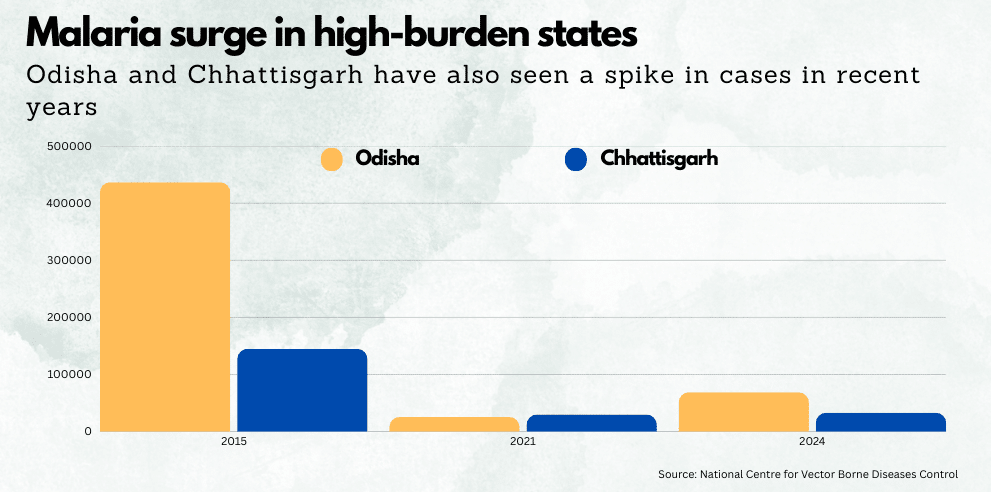
Malaria surge in high-burden states
Odisha and Chhattisgarh, two of India’s largest forested states, have historically borne a significant malaria burden. According to a statement by the government in 2020, regarding the then World Malaria Report, “(s)tates of Odisha, Chhattisgarh, Jharkhand, Meghalaya and Madhya Pradesh disproportionately accounted for nearly 45.47 percent (1,53,909 cases out of India’s 3,38,494 cases) of malaria cases … in 2019.”
However, both Odisha and Chhattisgarh had also seen a significant drop in malaria cases in the last decade, like the country- by about 84% and 77% respectively. However, both states have seen a rise in malaria cases from 2021 to 2024. While cases have only increased by about 11% in Chhattisgarh during this period, cases in Odisha have risen at a rate much higher than the national average—by over 84%.
Dr Yogesh Jain, a community health doctor who practices in rural Chhattisgarh, attributed this resurgence to complacency following earlier successes. “We had let our guard down about malaria. The program started patting itself on the back…and now it’s hitting back,” he told First Check.
Dr John Oommen, who practiced community medicine in tribal areas of Odisha for three decades, noted that malaria follows cyclical patterns, with sharp declines often followed by rises, as seen in 2023 and 2024. He said that Dr Oomen climatic factors, and disruptions like COVID-19, which shifted healthcare priorities, could have also contributed to these numbers.
Elimination vs. control: need to reconsider strategy?
India’s national malaria program aims for elimination by 2030, meaning no new cases should occur. “Elimination requires completely different strategies than control…it means not even a single case should happen,” explained Dr Jain.
Chhattisgarh has implemented its own Malaria Elimination Programme, leveraging primary healthcare workers to conduct proactive door-to-door testing during peak transmission seasons. These workers also perform targeted testing following irregular rainfall patterns in atypical months to ensure early case detection and prompt treatment. Additionally, the programme focuses on distributing insecticide-treated bed nets and promoting community awareness about preventive measures to curb malaria transmission effectively.
However, both experts argue that this “elimination” approach may not suit high-burden states.
Dr Jain said that as the entire focus is on elimination, resources get spread thinly across all areas, diluting efforts in high-burden regions.
“The states get shortchanged when the elimination strategy is implemented,” he said.
In contrast, control focuses on reducing deaths and transmission without chasing every case. For states like Odisha and Chhattisgarh, where malaria remains prevalent, a control strategy may be more practical. Odisha’s flagship Durgama Anchalare Malaria Nirakaran (DAMaN) programme appears to be more aligned with this strategy and drives comprehensive malaria control through mass testing, timely treatment, and widespread distribution of insecticide-treated bed nets.
Dr Oommen emphasized the need for micro-targeting, with district- and block-level plans tailored to local conditions in the state. He cited Odisha’s success with the DAMAN program in 2017–2019, which combined mass screening, treated bed nets, and village-level interventions to achieve an 80% reduction in cases.
Preventive measures, particularly insecticide-treated bed nets, are critical to malaria control. However, both states face challenges in ensuring their availability and use. In Chhattisgarh, Dr Jain noted that bed nets have not been distributed since 2018, and even then, coverage was limited to high-burden areas.
“Their (bed nets) life is not more than three years,” he said, highlighting the gap in replacements. Dr Oommen echoed this concern, stating that the supply of treated nets, often funded externally, remains inconsistent. “The single most important thing in the prevention strategy is provision and utilization of treated nets,” he said.
Beyond nets, other preventive strategies, such as repellents and prophylactic drugs, are underutilized due to logistical challenges and competing healthcare priorities, according to the experts. Dr Jain pointed out that as malaria cases declined, the disease received less attention, leading to reduced investment in prevention. In Odisha, while the DAMAN program showed success, its momentum has waned, with Dr Oomen urging a revival of its strategies.
Need for reliable data, training and coordination.
Effective surveillance is the backbone of malaria control, enabling early detection and intervention. India’s malaria report highlights a rise in the Annual Blood Slide Examination Rate, but both experts said that systemic flaws hinder this.
In Chhattisgarh, Dr Yogesh described a weak surveillance system hampered by disincentives to report cases. “The same people responsible for surveillance are also running the program…if you report more problems, it means you didn’t do your work well,” he explained, underlining how this could lead to underreporting.
In Odisha, Dr Oommen emphasized the need for real-time, reliable data to support elimination as well. “Without that, you can’t eliminate,” he said, noting that information management has been a persistent challenge.
A skilled and motivated workforce is essential for malaria control, but both states face shortages. While Odisha’s surveillance system, supported by Accredited Social Health Activists (ASHAs), is designed to test all fever cases within 24 hours, implementation varies due to stock-outs, worker shortages, and logistical barriers in remote tribal areas, Dr Oommen noted.
“Malaria disproportionately affects the most remote and marginalized communities, like poor and Adivasi populations, which is why strong political commitment is essential to address their neglect,” Dr Yogesh emphasized, adding how such areas are underserved.
Interstate coordination is another weak link— while many of the high burden states such as Chhattisgarh, Odisha, Jharkhand and Madhya Pradesh, are geographically close and dealing with similar issues, Dr Jain dismisses the idea of collaboration between the states as a “pipe dream,” citing budget constraints and differing priorities. Migration, particularly of seasonal laborers, further complicates efforts, as travelers from high-burden areas can spark outbreaks elsewhere. Testing all travelers, as recommended, is rarely implemented.
Looking forward: The next chapter in India’s malaria story
A 2022 study in The Lancet Regional Health – Southeast Asia highlights that India faces several challenges and roadblocks in its journey towards malaria elimination by 2030. “The challenges are incomplete paper based aggregated surveillance, missing private sector involvement, lack of a platform for digital integration of data and the need for more sensitive diagnostic tools,” the study concluded.
The study also warns of the threats of drug and insecticide resistance and notes that outdoor transmission of malaria and behavioral change of vectors make current vector control tools less effective. India nearly eradicated malaria in the 1960s, with cases dropping to under 50,000 in 1961 due to the success of the National Malaria Control Programme. However, complacency and emerging resistance to chloroquine and DDT led to a dramatic resurgence, with cases soaring by the mid-1970s.
Dr Oomen warned of the looming threat of a similar drug resistance, which could derail progress. Artemisinin-based combination therapy (ACT) is effective for P. falciparum, but availability is inconsistent. For P. vivax, which is rising in prevalence, treatment requires a 14-day course of primaquine, which patients struggle to complete.
Climate change is also a threat multiplier and could undo the progress already made in controlling malaria, especially in endemic areas. According to a WHO study titled Quantitative Risk Assessment of the Effects of Climate Change on Selected Causes of Death, 2030s and 2050s, climate change is projected to significantly exacerbate malaria mortality, potentially leading to an additional 60,000 deaths per year during the 2030s and 2050s.
Intensified rainfall and prolonged droughts can lead to more stagnant water pools, expanding breeding grounds for malaria-carrying mosquitoes. Higher temperatures can also speed up the maturation of the Plasmodium parasite inside these vectors, heightening the risk and intensity of malaria transmission.
These concerns are not lost on the experts.
“If this year is worse than 2024, and 2024 was worse than 2023, then I’d clearly say [in] 2030 [elimination] is not likely to happen,” said Dr Jain.